Svennberg E et al.: Clinical outcomes in systematic screening for atrial fibrillation (STROKESTOP): a multicentre, parallel group, unmasked, randomised controlled trial. The Lancet 398 (2021): 1498-1506. doi.org/10.1016/S0140-6736(21)01637-8
Auf dem EHRA-Kongress 2021 stellte Emma Svennberg die Ergebnisse der STROKESTOP-Studie vor, die 2012-2014 in Schweden durchgeführt wurde: Alle 75- und 76-Jährigen mit Wohnsitz in den Regionen Halland und Stockholm sind nach dem Zufallsprinzip zu einem Screening auf Vorhofflimmern (n=14.387) oder zu einer Kontrollgruppe (n=14.381) eingeladen worden. Die Screening-Gruppe wurde in lokalen Zentren untersucht und jene ohne VHF-Anamnese wurden gebeten, 14 Tage lang 2x täglich mit einem Device (Zenicor-EKG) intermittierende EKG aufzuzeichnen. Wenn anamnestisch oder bei den EKG-Aufzeichnungen VHF festgestellt, wurde eine orale Antikoagulantien angeboten. Alle Teilnehmer wurden mindestens 5 Jahre lang hinsichtlich des primären kombinierten Endpunkts (Schlaganfall, systemische Embolie, klinikpflichtige Blutung oder Tod jedweder Ursache) weiterverfolgt.
Quelle: Svennberg E auf Youtube
Quelle: Svennberg E auf Youtube
Abstract
Background
Atrial fibrillation is a leading cause of ischaemic stroke. Early detection of atrial fibrillation can enable anticoagulant therapy to reduce ischaemic stroke and mortality. In this randomised study in an older population, we aimed to assess whether systematic screening for atrial fibrillation could reduce mortality and morbidity compared with no screening.
Methods
STROKESTOP was a multicentre, parallel group, unmasked, randomised controlled trial done in Halland and Stockholm in Sweden. All 75–76-year-olds residing in these two regions were randomly assigned (1:1) to be invited to screening for atrial fibrillation or to a control group. Participants attended local screening centres and those without a history of atrial fibrillation were asked to register intermittent electrocardiograms (ECGs) for 14 days. Treatment with oral anticoagulants was offered if atrial fibrillation was detected or untreated. All randomly assigned individuals were followed up in the intention-to-treat analysis for a minimum of 5 years for the primary combined endpoint of ischaemic or haemorrhagic stroke, systemic embolism, bleeding leading to hospitalisation, and all-cause death. This trial is registered with ClinicalTrials.gov, NCT01593553.
Findings
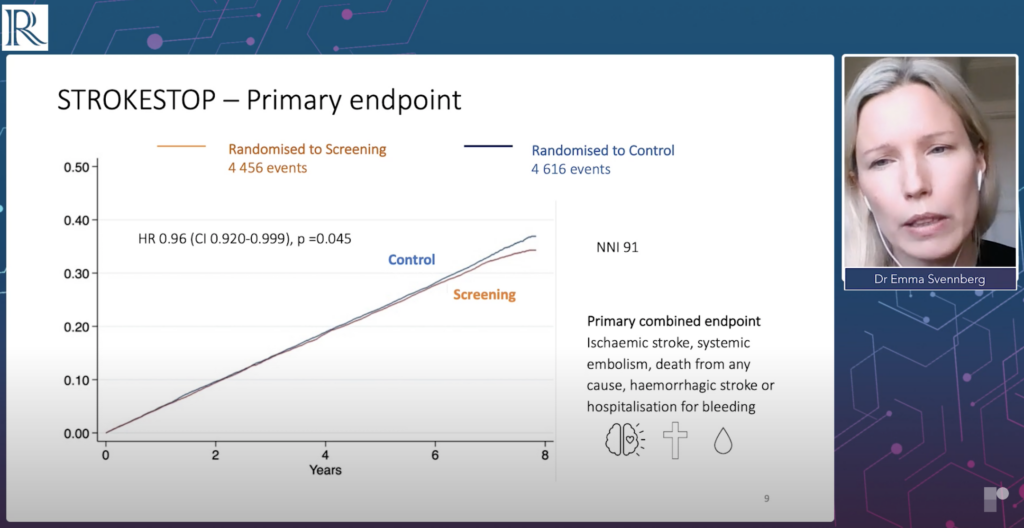
From March 1, 2012, to May 28, 2014, 28 768 individuals were assessed for eligibility and randomly assigned to be invited to screening (n=14 387) or the control group (n=14 381). 408 individuals were excluded from the intervention group and 385 were excluded from the control group due to death or migration before invitation. There was no loss to follow-up. Of those invited to screening, 7165 (51·3%) of 13 979 participated. After a median follow-up of 6·9 years (IQR 6·5–7·2), significantly fewer primary endpoint events occurred in the intervention group (4456 [31·9%] of 13 979; 5·45 events per 100 years [95% CI 5·52–5·61]) than in the control group (4616 [33·0%] of 13 996; 5·68 events per 100 years [5·52–5·85]; hazard ratio 0·96 [95% CI 0·92–1·00]; p=0·045).
Interpretation
Screening for atrial fibrillation showed a small net benefit compared with standard of care, indicating that screening is safe and beneficial in older populations.